Positional plagiocephaly
OVERVIEW
What is positional plagiocephaly?
Positional plagiocephaly, also known as positional flat head, positional brachycephaly, or deformational plagiocephaly, refers to a condition primarily occurring in infancy, most commonly between 7 to 12 weeks of age. It is caused by prolonged pressure on the skull due to positioning, leading to an asymmetrical, flattened, or misshapen head—commonly referred to as a "flat head" or "flattened skull." This differs from the aesthetically preferred "round head." The more accurate medical term is "positional skull deformity."
Since the 1990s, there has been an increase in reported cases of skull asymmetry in children, particularly occipital flattening (flat head). This may be linked to the American Academy of Pediatrics (AAP) recommendation for infants to sleep on their backs. While back sleeping carries some risk of skull deformation, it significantly reduces the incidence of sudden infant death syndrome (SIDS).
Positional plagiocephaly typically peaks at around 4 months of age and begins to improve noticeably by 6 months. Therefore, skull deformities caused by external factors—such as prolonged supine positioning without adequate tummy time or movement—are usually benign and reversible.
Over 80% of infants with positional skull deformities develop a "round head" by the age of 2. This condition does not affect brain development or intelligence and does not require surgical intervention, distinguishing it from pathological skull deformities caused by craniosynostosis.
SYMPTOMS
What are the symptoms of positional plagiocephaly?
Positional plagiocephaly, as the name suggests, refers to a flattening of the skull, which is normally round, occurring on one or multiple sides simultaneously.
As shown in the diagram of a newborn's fontanelles and cranial sutures (Figure 1), before the fontanelles and sutures close, uneven or multidirectional pressure can cause varying degrees of flattening on the affected side of the skull, leading to cranial deformities. This results in different head shapes such as flat head, oblique head, asymmetrical head, brachycephaly, or scaphocephaly (similar to the shapes in Figure 2).
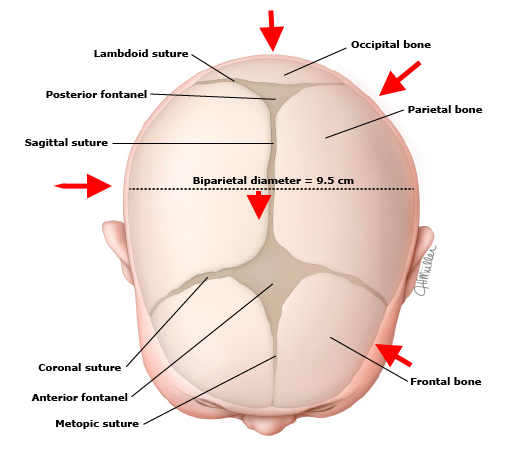
(Figure 1 source: UpToDate Clinical Advisor)
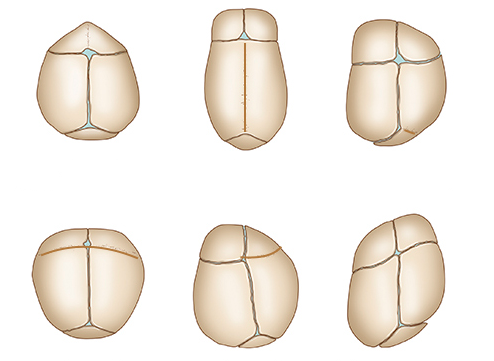
(Figure 2 source: UpToDate Clinical Advisor)
The most common positional cranial deformity is flattening of the occipital bone (back of the head), followed by flattening or tilting of the temporal region (the side of the head near the ears). Other areas of the skull may also become flattened or asymmetrical. In some cases, the top of the head may flatten, known as positional brachycephaly, where the skull shortens in length and widens in the front-back or left-right directions.
CAUSES
What causes positional plagiocephaly?
-
Most skull deformities observed at birth, such as flattening of the occipital bone or cranial asymmetry, may be caused by mechanical forces acting on the head in the uterus or during delivery. Common causes include uterine contractions, prolonged labor, birth canal compression, multiple births, post-term pregnancy, oligohydramnios, breech or transverse position, or assisted delivery methods like forceps or vacuum extraction. Most of these deformities improve on their own within a few months after birth.
-
Positional skull deformities that occur after birth are primarily due to prolonged supine sleeping or lying flat during the day, where sustained pressure on a fixed position of the skull leads to deformities, with occipital flattening being the most common. These deformities may improve naturally or can be corrected through proper education, positional changes, postnatal activities, and external shaping. If skull deformities occur without pressure-related causes or are atypical, non-positional pathological factors should be ruled out.
What are the physiological characteristics of a newborn or infant's skull?
A newborn's skull consists of bone plates separated by sutures, making it soft and elastic, easily deformable under pressure. The skull can temporarily deform during birth, facilitating smooth delivery and accommodating future brain growth (Figure 3).
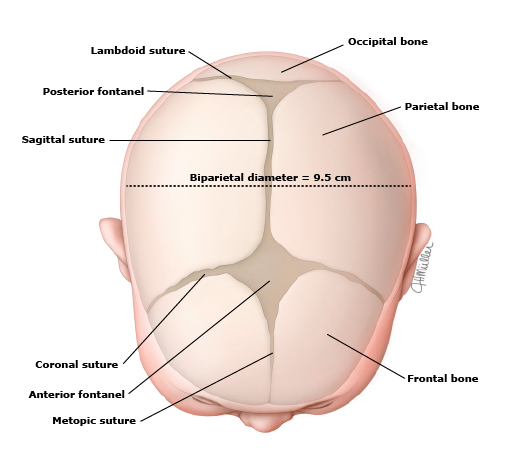
(Figure 3 source: UpToDate Clinical Advisor)
The fontanelles and cranial sutures in infants and young children close in a specific manner and timeframe:
-
The posterior fontanelle usually closes within 2 months after birth, while the anterior fontanelle typically closes before 2 years of age.
-
The horizontal and vertical sutures shown in Figure 3 generally close between 22 to 26 months.
-
In preterm infants, fontanelle closure is often delayed, while the growth of scalp muscle fibrous tissue may precede fontanelle closure by several months.
-
Sutures in the palate, frontonasal, and parietozygomatic regions do not close until adulthood, after craniofacial growth is complete.
Can the head shape of a baby with positional plagiocephaly still change?
Yes, it can change. Head circumference continues to grow into adulthood. For example, the Conehead tribe in Africa shapes their heads through postnatal methods. The faster the head circumference grows, the more noticeable the changes in head shape.
Due to the physiological characteristics mentioned above, fibrous tissue growth may sometimes make it seem like a baby's fontanelles or sutures have "closed" upon touch, but this may not be the case. Even if the major fontanelles and sutures close, other sutures that cannot be felt remain open, allowing head circumference to continue growing into adulthood.
A 2004 study showed that the prevalence of positional skull deformities at 6 weeks, 4 months, 8 months, 12 months, and 24 months was 16%, 20%, 9%, 7%, and 3%, respectively, indicating that head shape gradually changes during natural growth and tends to return to the innate "round head" shape.
However, a very small number of children with positional plagiocephaly may retain the condition into adolescence or even adulthood.
Another 2013 study found that the prevalence of positional plagiocephaly at 7–12 weeks was 47%, which may be related to the American Academy of Pediatrics' recommendation for supine sleeping in infants.
Overall, before the age of 2, especially before 1 year when head circumference grows the fastest, infants and young children still have significant potential for head shape remodeling.
DIAGNOSIS
How is positional plagiocephaly (positional skull deformity) diagnosed?
Positional plagiocephaly is primarily diagnosed clinically based on birth conditions (head shape at birth may also be affected by scalp hematoma or caput succedaneum), postnatal progression of head shape changes, and physical examination.
-
Ear position is the most commonly used physical examination criterion for diagnosing positional plagiocephaly. In positional plagiocephaly, the ear deviates from the flattened area (see Figure 4, right);
-
Cranial ultrasound or skull X-rays can help exclude craniosynostosis as a cause of skull deformity;
-
CT scans are not routinely used to diagnose positional plagiocephaly. This test is only performed when medical history, clinical examination, and ultrasound cannot confirm the specific condition, and further evaluation of cranial sutures, brain anatomy, or other potentially abnormal structures is required.
What conditions should positional plagiocephaly be differentiated from?
-
Congenital torticollis: Congenital torticollis may also lead to positional plagiocephaly, mainly due to restricted head and neck rotation, causing persistent tilting to one side. Most children with congenital torticollis exhibit visible craniofacial asymmetry, while a few cases are less obvious. Differentiation is made through physician examination and neck muscle ultrasound.
-
Positional torticollis: Similar to positional plagiocephaly, it is caused by postural preference, which can also induce positional plagiocephaly (plagiocephaly). Differentiation is made through physician examination and neck muscle ultrasound.
-
Skull deformities caused by craniosynostosis: Craniosynostosis restricts skull growth direction, leading to skull deformities that resemble positional plagiocephaly. Differentiation can be assisted by medical history, physical examination, ultrasound, skull X-rays, or CT scans.
-
As shown in Figure 4, in posterior positional plagiocephaly, the ear deviates from the flattened area, shifting forward (Figure 4, right). In contrast, in posterior craniosynostosis-related plagiocephaly, ear position may be symmetrical, though in some cases, it may deviate toward or away from the fused suture side.
-
Additionally, when viewed from above, positional plagiocephaly forms an approximate parallelogram (Figure 4, right), with the ipsilateral ear shifted forward. Besides unilateral flattening of the occipital region, there is also ipsilateral frontal/parietal (forehead) bossing and zygomatic prominence.
-
If the diagnosis of positional plagiocephaly is uncertain, skull X-rays or ultrasound can confirm that the cranial sutures are open.
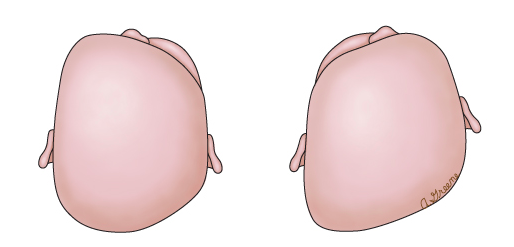
(Figure 4 source: UpToDate Clinical Advisor)
TREATMENT
Which department should I visit for positional plagiocephaly?
Pediatrics, Child Health, Pediatric Neurosurgery, Pediatric Craniofacial Surgery
How is positional plagiocephaly treated?
Current treatments for positional plagiocephaly mainly include: positional correction, adjustment and exercise of force direction, cranial orthosis (helmet), and surgical correction.
Positional correction, both preventive and therapeutic
- Have the baby sleep in the supine position, alternating the head tilt to the left and right (i.e., alternating pressure on the back of the head).
- When the baby is awake during the day, ensure at least 30–60 minutes/day of tummy time, with each session adjusted according to the baby's ability. Parents should supervise for safety, and the tummy time mat should be firm, not too soft, to avoid affecting the baby's body control and support.
- Apart from sleeping or going out, minimize opportunities for the baby to remain in the supine position, such as in strollers, cradles, or baby swings.
Daily tummy time not only prevents positional plagiocephaly or slows its progression but also improves developmental quotients in infants under 15 months. When the baby can sit and crawl around 6 months, reduced awake supine time and correction of torticollis can significantly improve positional plagiocephaly.
Adjustment and exercise of force direction
- If plagiocephaly has already occurred, adjust the baby's sleeping position so the rounded part of the head rests on the mattress, while the flattened part is kept away from it.
- Reposition the crib to encourage the baby to turn their head toward the non-flattened side to see parents or objects in the room.
- If the baby has torticollis, simultaneous intervention is needed to reduce time spent with the head tilted toward the flattened side. Postural torticollis requires appropriate neck nodding exercises to relieve muscle stiffness. If necessary, consult a child health specialist for professional therapy.
- Increase tummy time as much as possible based on the baby's condition.
Cranial orthosis (helmet)
- Since most infants improve by 6 months, the above two steps should be tried for babies under 6 months.
- If parents perceive severe plagiocephaly or a pediatrician/child health specialist recommends referral, an experienced pediatric neurosurgeon or craniofacial surgeon should evaluate, diagnose, and guide further management, including cranial orthosis (helmet) or surgery.
- For severe deformities or moderate/severe cranial deformities in infants older than 6 months without improvement, orthotic helmets are recommended.
- The optimal age for helmet use is 4–12 months, as the skull is more malleable, brain growth is rapid (aiding normalization), and infants adapt better to wearing helmets. However, improvement is still possible after 12 months.
- Helmets require regular adjustments by specialists to accommodate skull growth and shape changes.
- Other methods like shaping pillows, though effective, are not recommended for home use due to increased risk of sudden infant death.
Surgical correction
- Surgical intervention is rarely needed for positional plagiocephaly, except in severe, uncommon cases, which require evaluation and treatment by a pediatric neurosurgeon or craniofacial surgeon.
DIET & LIFESTYLE
What dietary precautions should be taken for positional plagiocephaly?
There are no specific dietary restrictions; maintaining a healthy and balanced diet is sufficient. A daily vitamin D supplement of 400 IU is recommended. Follow medical advice for special circumstances.
What lifestyle precautions should be taken for positional plagiocephaly?
No special lifestyle precautions are needed—maintaining a healthy routine is sufficient. Actively encouraging an infant's gross motor skills can help prevent positional plagiocephaly.
PREVENTION
Can Positional Plagiocephaly Be Prevented?
Most cases can be prevented.
-
Follow standardized prenatal care during pregnancy to reduce avoidable abnormal deliveries.
-
Refer to point 1 in the treatment plan—it serves as both treatment and prevention.